
Levels of Scientific Evidence: A Complete Guide for Researchers and Professionals
In clinical research and evidence-based practice, not all data carries the same weight. Professionals must routinely grade the quality of information to make safe, data-driven decisions. Understanding the levels of scientific evidence is the foundation of this process. This framework provides a structured hierarchy that ranks research designs based on their freedom from bias. Navigating this hierarchy allows researchers, clinicians, and policy experts to distinguish between weak anecdotes and robust, rigorous conclusions. You can explore official methodological standards via the Oxford Centre for Medicine to see how these frameworks function in practice.
This comprehensive guide breaks down the evidence pyramid from top to bottom. We will examine each tier, explore its practical applications, and discuss how to apply these frameworks effectively.
Understanding the Evidence Hierarchy and Study Designs
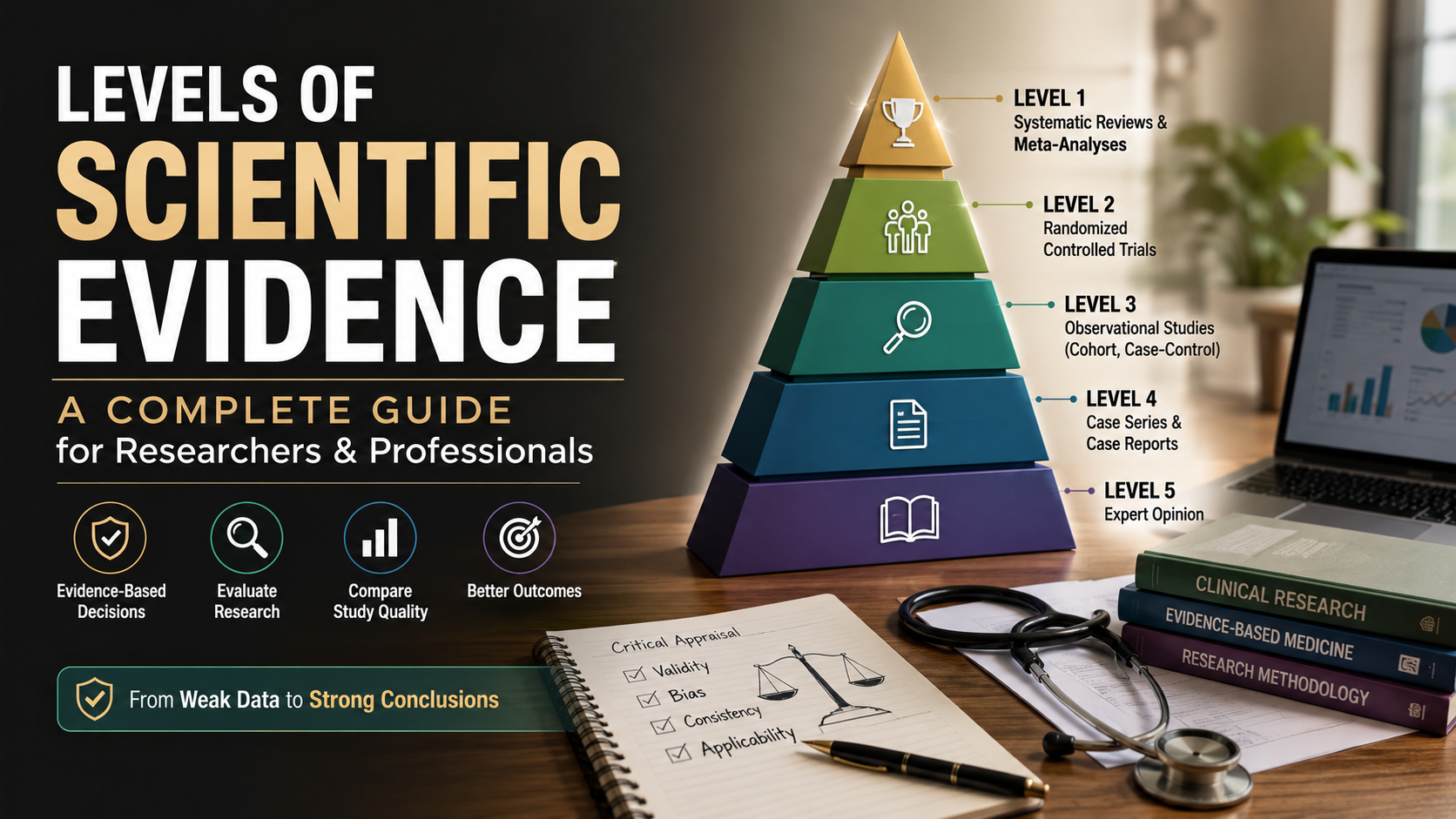
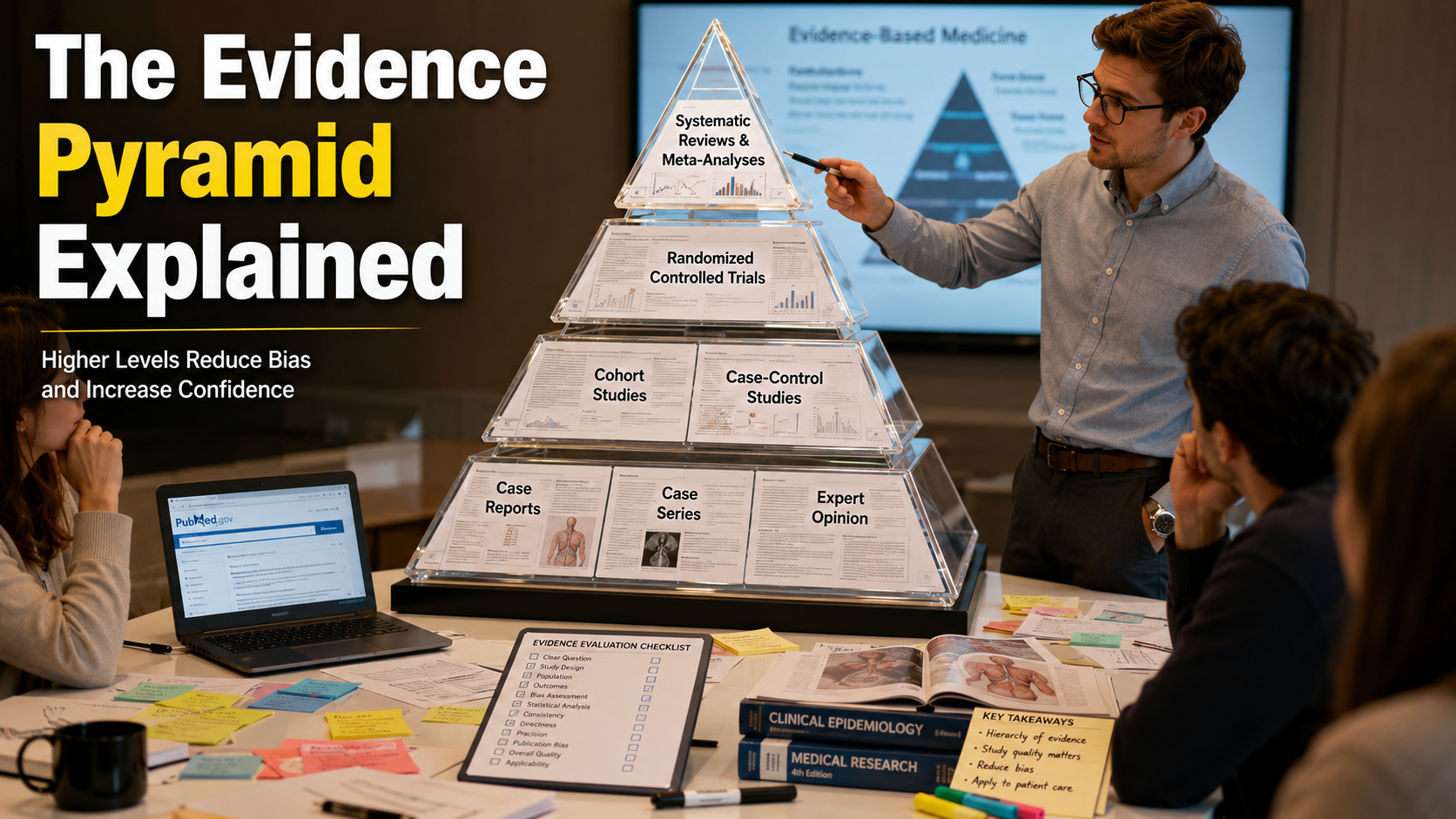
The hierarchy of research validation visually resembles a pyramid. At the broad base, you find studies with higher risks of bias. However, these foundational levels still provide valuable preliminary insights. As you move toward the peak, the study designs become more rigorous. These higher tiers control for confounding variables much more effectively. Healthcare and scientific communities rely on this ranking system daily. The structure helps them translate complex laboratory findings into safe, everyday practices. By understanding where a study sits on this pyramid, professionals can mitigate risk and avoid over-interpreting preliminary results.
Understanding this system prevents professionals from falling victim to sensationalized headlines. Often, a breakthrough reported in the media stems from a preliminary animal study or a small case series. While these foundational discoveries are exciting, they represent the earliest stages of scientific validation. A truly dependable clinical intervention requires confirmation from the upper tiers of the pyramid. In those stages, researchers deliberately design experiments to eliminate human error and chance. Consequently, mastering this structural framework elevates your ability to critique literature, design better institutional protocols, and allocate research resources efficiently.
The Tiers of the Levels of Scientific Evidence

To properly evaluate data, we must analyze the specific tiers that comprise the levels of scientific evidence. Each level serves a distinct purpose in the broader research ecosystem, offering varying degrees of predictive power and reliability.
Level 1: Systematic Reviews and Meta-Analyses (Peak Research Validation)
Systematic reviews sit at the very peak of the scientific hierarchy. These papers do not conduct new experiments from scratch. Instead, authors collect, appraise, and synthesize all existing high-quality studies on a specific topic. When researchers combine the statistical power of multiple independent studies, it is called a meta-analysis. This process offers the highest level of certainty because it irons out the statistical anomalies of smaller, isolated trials.
By pooling data from thousands of participants across different global sites, a meta-analysis can reveal subtle patterns. A single localized trial might completely miss these trends. This methodology reduces the impact of publication bias and provides a highly objective overview of current knowledge. For policy makers and clinical directors, Level 1 evidence serves as the definitive bedrock for building gold-standard guidelines. It minimizes the risk of relying on anomalous, unreplicable research anomalies.
Level 2: Randomized Controlled Trials (The Gold Standard Experimental Design)
Randomized controlled trials are the gold standard for primary experimental research. In an RCT, investigators randomly assign participants to either an experimental group or a control group. This random allocation ensures that baseline characteristics remain balanced between groups. Consequently, any differences in the final outcome stem from the intervention itself rather than external variables. Researchers often utilize blinding protocols, ensuring that neither the patients nor the doctors know who receives the active treatment.
Blinding prevents psychological expectations from skewing the objective physical results of the trial. The rigorous structure of an RCT allows investigators to establish clear cause-and-effect relationships with high internal validity. However, these trials remain incredibly expensive, time-consuming, and logistically complex to execute properly. Despite these operational hurdles, the scientific community treats well-conducted RCTs as the essential benchmark that an intervention must pass before widespread adoption or regulatory approval occurs.
Level 3: Observational Studies (High-Quality Cohort and Case-Control Data)
When experimental manipulation is unethical or impractical, researchers turn to observational designs. Cohort studies follow a group of individuals forward in time to see how specific exposures affect their health or behavior. Conversely, case-control studies work backward, identifying individuals with a specific outcome and looking into their past to find common exposures. While highly informative, these designs cannot definitively prove causation because they lack random assignment.
For example, tracking the long-term health effects of smoking relies entirely on observational studies. Forcing a random group of people to smoke for decades would be a massive ethical violation. Despite the lack of experimental control, observational studies excel at identifying long-term epidemiological trends. They also spotlight potential risk factors in massive populations over multiple generations. They provide essential real-world context that tightly controlled laboratory environments sometimes fail to capture, making them foundational to public health tracking.
Level 4: Case Series, Case Reports, and Expert Opinion (Foundational Insights)
At the base of the human clinical evidence pyramid are case reports and expert opinions. A case report describes the unique symptoms, treatment, or clinical course of a single patient. A case series aggregates a small cluster of similar cases. While these publications offer critical early warnings for new diseases or unexpected drug side effects, they possess high susceptibility to bias. Therefore, they suggest possibilities rather than establishing definitive medical truths.
Expert opinions, though delivered by seasoned professionals with decades of field experience, sit at the bottom. They lack systematic empirical validation. An expert’s perspective can be influenced by personal anecdotes, institutional traditions, or individual cognitive biases. Nevertheless, this base layer remains crucial for innovation. It serves as the primary incubator for new hypotheses, highlighting unusual medical anomalies that spark the grand experimental trials found in the upper echelons of the evidence pyramid.
Grading Research Quality for Professional Decision-Making
Applying the levels of scientific evidence requires a balanced perspective. While top-tier data is ideal, researchers must often work with the best available data given ethical and financial constraints. For instance, testing a toxic substance on humans in an RCT is entirely unethical. In such scenarios, well-designed cohort studies represent the highest ethical tier available. Professionals must learn to judge the quality of execution within each specific study type, ensuring that minor design flaws do not undermine the conclusions.
Furthermore, implementing evidence-based practice means integrating this hierarchy with real-world clinical expertise and unique patient values. A perfect Level 1 meta-analysis might recommend a specific drug. However, if that medication is prohibitively expensive or unavailable in a rural setting, the professional must pivot. They must evaluate lower-level studies to find a viable, secondary alternative that remains safe and effective. Balancing the ideal purity of the evidence pyramid with the practical realities of fieldwork is what distinguishes a truly masterful researcher from a rigid theoretician.
FAQ Section
What are the levels of scientific evidence?
The levels of scientific evidence form a graded ranking system used to evaluate the quality, validity, and bias risk of research studies. Structured as a pyramid, this framework places systematic reviews and randomized controlled trials at the peak due to their strict controls and low susceptibility to error. Conversely, observational studies, case reports, and expert opinions sit closer to the base.
Professionals utilize this hierarchy to determine how much weight to give specific findings when making clinical, scientific, or policy decisions. By standardizing how data is critiqued, the global scientific community can easily identify which conclusions are backed by robust empirical numbers and which require further validation. It essentially acts as a quality assurance filter, ensuring that high-stakes choices, such as approving a new pharmaceutical drug or shifting environmental regulations, are anchored in the most flawless methodologies available.
Why is the hierarchy of evidence important in research?
This hierarchy is crucial because it protects professionals from making critical decisions based on flawed, biased, or accidental data. Not all research is conducted with the same rigor, and smaller studies can easily produce deceptive findings due to random chance or hidden confounding variables. By utilizing a standardized ranking system, researchers can quickly categorize the strength of a study’s architecture.
It creates a universal language for data verification across vastly different scientific fields, from agriculture to medicine. Without this hierarchy, an individual anecdote could be given the same institutional weight as a massive trial involving thousands of people. The pyramid ensures that scientific progress moves forward systematically, anchoring major societal advancements to reproducible, transparent, and mathematically sound experimental frameworks rather than relying on mere guesswork or localized coincidences.
Can a lower-level study ever be more valuable than a higher-level one?
Yes, lower-level studies can be significantly more valuable depending on the context, ethical boundaries, and specific clinical questions asked. For rare diseases affecting only a handful of people worldwide, conducting a massive randomized controlled trial is mathematically and logistically impossible. In these specific scenarios, a meticulous case series or a small case-control study provides invaluable clinical insights that a flawed or underpowered trial cannot replicate.
Furthermore, during the early days of an emerging pandemic, clinicians cannot afford to wait years for a systematic review to be organized and published. They must rely on rapid case reports and expert opinions to share immediate, real-time treatment strategies on the ground. Therefore, the ultimate utility of the data always depends on ethical boundaries, temporal urgency, and the unique nature of the professional inquiry.
What is the main difference between a systematic review and a meta-analysis?
A systematic review is a comprehensive qualitative summary of existing literature that answers a specific research question using rigorous screening criteria. The authors define a strict search strategy to find every single paper relevant to their topic, filtering out poorly designed experiments to minimize bias. A meta-analysis takes this exact process a step further by using advanced mathematical methods to pool and recalculate the quantitative raw data from those selected studies.
It treats the combined papers as one massive mega-study, running fresh statistical tests to find definitive mathematical trends. In short, all meta-analyses are embedded within systematic reviews, but a systematic review can stand alone without a meta-analysis if the underlying data is too diverse to combine mathematically. Both represent the pinnacle of data synthesis but utilize different analytical toolsets.
How does bias affect the different levels of scientific evidence?
Bias affects research designs differently based on how much control investigators have over external variables and human behavior. Lower tiers, such as case reports or observational studies, lack random assignment, making them highly vulnerable to confounding variables, patient memory errors, and researcher subjectivity. If a patient is asked to recall their diet from ten years ago, their memory will naturally introduce significant errors into a case-control study.
Higher tiers implement strict randomization, double-blinding protocols, and standardized data synthesis to actively minimize these distortions. By ensuring that neither the researcher nor the subject can accidentally influence the data collection process, higher-level designs eliminate placebo effects and human partiality. This structural defense mechanism results in highly reliable, objective, and reproducible conclusions that can be confidently generalized to the public.
Conclusion
Navigating the levels of scientific evidence is an essential skill for any modern researcher, healthcare provider, or industry professional. By understanding the distinct tiers of the evidence pyramid, professionals can accurately appraise data, filter out weak methodologies, and apply robust insights to their daily work. While systematic reviews and randomized controlled trials remain the gold standard for establishing true causation, observational studies and case reports still provide crucial building blocks for scientific discovery. No single layer of the pyramid is useless. Rather, each design serves a specific phase in the lifecycle of knowledge generation.
Ultimately, maintaining a critical eye and respecting the hierarchy of research validation ensures safer practices, better policy decisions, and more accurate scientific advancements worldwide. As data continues to grow exponentially, the ability to sort high-quality evidence from weak data will remain a superpower. Understanding the core parameters of research-based vs evidence-based methodologies allows you to apply these insights contextually. Embracing this framework protects your projects from bias, enhances institutional credibility, and keeps your practices firmly rooted in empirical truth.